A new article published August 5 in Nature Human Behaviour integrates anonymized real-time mobility data with census and demographic data to model COVID-19 transmission in the Boston area.
The authors, including Esteban Moro, Visiting Professor in the Media Lab and IDSS, and Professor Sandy Pentland of MIT’s Connection Science Group, found that a period of strict social distancing, followed by robust testing, contact tracing and quarantine by household rather than individual could keep the disease’s impact manageable, while enabling broad reopening of economic activities.
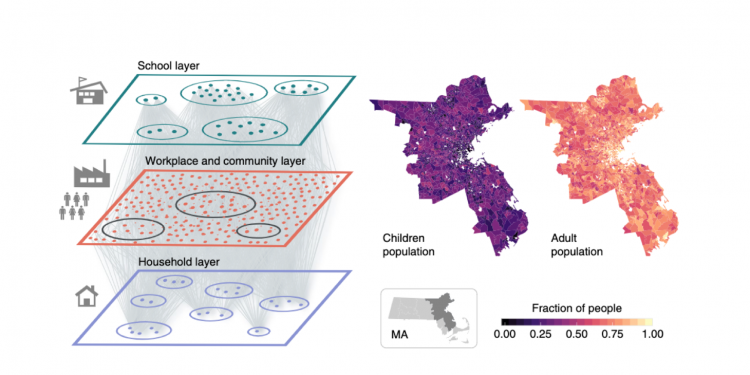
This research sheds new light on possible pitfalls and solutions as cities look to lift restrictions that have been in place throughout the summer in many locations. Using data from approximately 85K people in the greater Boston area, combined with known information about COVID-19 transmission rates, duration of stages, and other data points, the authors developed a complex model that can predict the number of new cases and hospitalizations under various scenarios of lifted restrictions.
Perhaps not surprisingly, in establishing a baseline, the study found that unmitigated lifting of restrictions would likely lead to a “second wave” that would quickly overwhelm Boston’s health care facilities, with peak of daily incidence of 25.2 newly infected individuals per 1,000 people, leading to a need for about 12 times the available ICU beds.
A second scenario, referred to as LIFT, assumed an additional 8 weeks of stay-at-home order, followed by another four of partial reopening, including work and community spaces, but not full reopening of restaurants and other spaces with mass social gatherings. After the total 12-week period, there would be a full lifting of all restrictions. In the LIFT scenario, the modeled impact was still well beyond the capacity of health care facilities, with a need for over nine times the ICU beds available at the peak of the likely second wave, an unsafe and almost certainly deadly situation. This makes it clear that a return to business as usual simply is not possible without some additional measures.
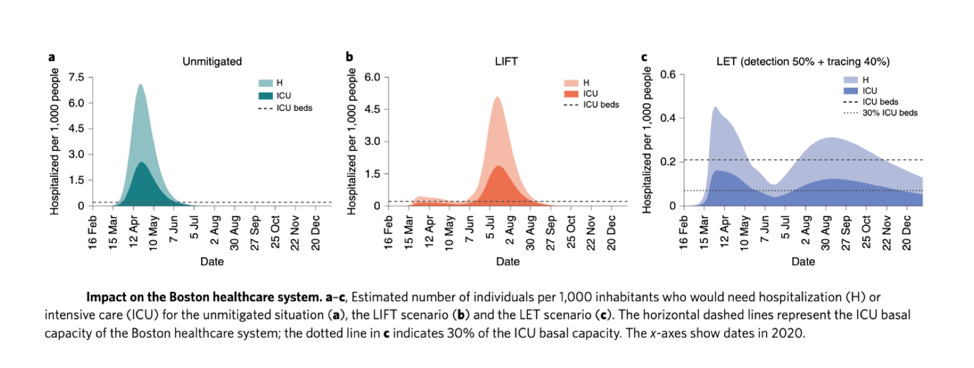
Short of a safe, effective, and widely utilized vaccine, there is no silver bullet that will allow the world to return to life as usual. However, the authors propose one possible solution to keep cases and hospitalizations manageable while allowing for a wide return to work and social activity. A third scenario involved the same LIFT measures described above plus robust testing, contact tracing of symptomatic people and quarantine of all household members of people who came in close contact with someone who tests positive for the virus. This is referred to as the LET scenario, short for Lift and Enhanced Tracing. After lifting of restrictions, at rates of 50% detection of positive cases within 2 days of onset of symptoms, tracing of 40% of contacts, and quarantine of all household members of those contacts, the model shows just .29 people per thousand in hospitals per day, compared with more than five per day under LIFT measures alone and more than seven under the unmitigated scenario. ICU beds would be more than adequate at all times under this scenario. Furthermore, the model assumes no additional precautions, such as masks and social distancing. Therefore, it is expected that new cases and hospitalizations could be even lower if people were to continue some of the practices that have helped combat the spread of COVID-19 thus far. The advantage of whole household quarantine is that it simplifies contact tracing, working at the level of small groups of people rather than individuals. Follow-up calls to check for compliance would also be streamlined.
This approach is not without sacrifice. The quarantining of full households presents unique challenges – it may be hard for quarantined families to obtain necessities, and quarantining together with others with known risk of infection may not be desirable. The study notes that at the peak, with 40% contact tracing, as many as 9% of all people in the city could be under quarantine. However, this number would gradually decline to around 3%. The total number in quarantine could be further reduced if testing ramps up more significantly. The authors suggest that the trade-off of higher numbers of people in quarantine compared with the massively disruptive long-term social isolation policies that would otherwise be needed to keep new infections manageable is well worth it. Life could return to some degree of normalcy, and the economy could begin to recover.
Since the study was carried out, Massachusetts has moved toward a manual tracing strategy in which thousands of people have been hired to trace potential infections. Esteban Moro explains that this could work if the number of cases is small and controlled, but it might be insufficient if the number of cases scales up. He also notes that hiring of contact tracers has been problematic.
Moro suggests a possible solution to deal with sudden growth in the number of cases is to combine manual and digital contact tracing (via an app), but he has not seen this widely discussed.
The model used in the study will continue to be developed and enhanced, and the authors plan to examine other cities beyond Boston. They will use real-time behavior data to investigate how infection is actually propagating and detect when, where, and why spreading events are happening.
Moro says, “If we want to rescale our lives, economy, and cities, we need to understand better how the infection is spreading across people and communities. Shutting down the whole economy and our cities because of a second wave might not be needed if we include accurate information about how people are behaving, moving, shopping, etc. in our society.”